What is a Meniscus Tear and Meniscus Repair?
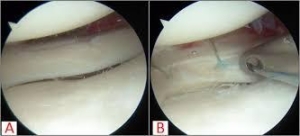
Lateral Meniscus Repair with PRP Injection(pre-surgery)
Surgery performed by Dr. Chams
Lateral Meniscus Repair with PRP Injection
Surgery performed by Dr. Chams
Lateral Meniscus Repair with PRP Injection(post-surgery)
Surgery performed by Dr. Chams
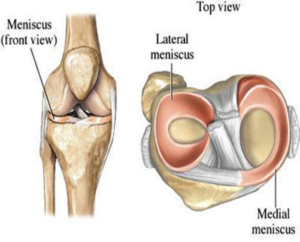
The knee is the largest and one of the most complex joints in the human body. It consists of 4 bones, multiple ligaments, muscles and tendons, cartilage and soft tissue. The boney structures of the knee consist of the patella (knee cap), Femur (thigh bone), Tibia and Fibula (lower leg bones). The smoothness motion of the knee is accomplished through articular cartilage and fibrocartilage. Articular cartilage is the protective covering over the ends of the bones. Meniscus is the additional form of cartilage within the knee called fibrocartilage. The purpose of your two meniscuses (medial – inside and lateral – outside) is to act as cushions between your femur (thigh bone) and tibia (lower leg bone).
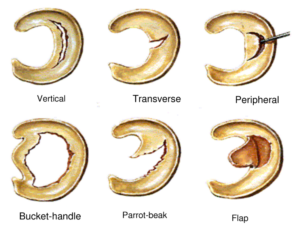
A meniscus tear is the most common injury in the knee and can occur at any age. Young athletes typically require a traumatic event to damage the meniscus. A meniscus tear, in this population, are usually associated with an additional injury such as an ACL tear or MCL tear. As we age, the menisci weaken increasing its chances to tear with repetitive activities. Meniscus tears are classified by the area of damage, length, width, and stability. Terms such as flap, transverse, peripheral, degenerative, anterior or posterior horn, horizontal cleavage, complex, parrot-beak and bucket handle describe the types of tears.
Signs and Symptoms
Signs and symptoms associated with meniscus tears include pain, swelling, instability episodes or feelings of instability, catching and locking. With specific types of tears, the knee may lose range of motion and lock without being able to gain full extension or full flexion. Typically straight ahead movement will not illicit symptoms. Twisting, squatting, lunging, cutting or planting will exacerbate symptoms.
Diagnosis
Diagnosis will be determined through a thorough history and physical examination by a trained sports medicine and orthopedic knee specialist. Examination will consist of palpating the knee complex for pain and a visual examination for deformities. The clinician will check both active and passive range of motion. Specific manual tests will be performed by the specialist to determine if inflammation exists, the amount of weakness, instability and other possible factors causing symptoms. Once the initial diagnosis has been made, radiological examinations may need to take place for further assessment. An MRI (3 dimensional picture) may be ordered to assist in determining the injury. X-rays of the knee complex may be ordered to determine the alignment the joint and rule out significant osteoarthritis as well as any additional bone conditions such as fracture or loose bodies prior to the MRI.
Non-Surgical Treatment or Conservative Management
Non-surgical treatment or conservative management goals are to decrease painful symptoms allowing individuals improved abilities to perform activities of daily living and labor tasks. Management consists of rest, change in activities, anti-inflammatory (NSAID) medications, Ice 20-30 minutes at times, physical therapy/home exercise program and possible injections of corticosteroid. If conservative treatment fails and individuals remain symptomatic, then proceeding with surgical management is required.
Surgical Management
Surgical management includes knee arthroscopy. Arthroscopy occurs when a small camera is placed into the knee joint to visualize the damage. During this visualization, ligaments, articular cartilage, meniscus and other soft tissue structures are evaluated. Once the assessment has been completed the surgeon uses a variety of instrumentation to repair, or debride (clean) the meniscus.
- A partial meniscectomy is the surgical removal of only the torn portion of the meniscus. The uninjured meniscus is left intact.
- A meniscus repair occurs when the surgeon places a stitch into the meniscus to prevent further tearing and promote healing. Through this repair, the entire meniscus is preserved.
Click for video demonstration with Fast Fix.
- A meniscal transplant replaces the damaged meniscus with a cadaver donor portion of meniscus. Transplants are not advocated for everyone. Active people younger than 55 years of age, a low BMI and individuals with minimal joint damage may be eligible for this type of treatment. Once a donor and size have been matched to the meniscal transplant recipient, a mini open incision is made and an arthroscopic camera is used to place anchors into Tibia (shin bone) and stitches into the allograft assist in stabilizing the transplant for healing. Post-operative care is long and challenging. It includes immobilization and non-weight bearing for 4-6 weeks. Physical therapy is performed to regain range motion, knee strength, and stability. Full release to work and play can be as early as 6 months and as long as 12 months.

Pre / Post Meniscus Transplant
Knee arthroscopy is an outpatient procedure. Recovery for knee arthroscopy for return to strenuous work and play activities for partial meniscectomies can vary from 4-8 weeks. The recovery for a meniscal repair includes 4-6 weeks of non-weight bearing in a brace and return to sports or activity around 4 months post-operative.
Rehabilitation
Rehabilitation, as stated above, recommend for both surgical and non-surgical management. Regardless of your treatment choice, your sports medicine physician will determine a personalized treatment program that fits your needs. This recovery process can be long and tasking. However, your active involvement will improve your recovery time. Initial goal following surgery is to reduce swelling and pain, increase mobility and range of motion. At home and at physical therapy, the use of ice, modalities and specific range of motion and strengthening exercises will be performed several times throughout the day. Pain and anti-inflammatory medication may also be prescribed for additional benefit. Crutches and bracing may be initialized following your assessment to aid in stability and prevent further damage to the knee complex. Once arthroscopic meniscectomy or repair takes place, physical therapy will begin the following day, working towards restoring full range of motion, strength, and stability of the knee complex. Advancement to a work specific or sports specific injury prevention program typically occurs around the 4-6 week mark for partial meniscectomies and the 3-4 month mark for meniscal repairs.