What is Shoulder Arthritis?
Total Shoulder Replacement
3D Surgical Animation
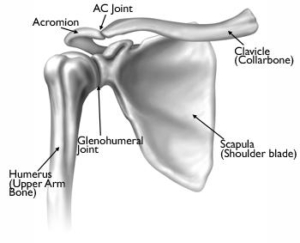
Although most people think of the shoulder as several joints, there are really two joints in the area of the shoulder. The shoulder complex is a ball and socket joint and is comprised of 4 main muscles, several bones, and several soft tissue structures. The scapula (shoulder blade), clavicle (collar bone), and humerus (upper arm bone) make up the bony components. The upper portion of your shoulder creates a joint between the clavicle and scapula called your AC joint – acromioclavicular. Your glenohumeral joint is created from the ball (head of the humerus) and socket (glenoid fossa). Covering of each bone consists of articular cartilage (white protective covering) that breaks down within this condition. When osteoarthritis the protective lining of the bone decreases it produces the bones to compress and rub.
There are several types of arthritis and your physician will need to determine which joint is affected and by which type of arthropathy. Osteoarthritis or “wear and tear” by definition is inflammation of a joint. Within the shoulder complex, this can occur at either your AC joint and or your glenohumeral joint. Osteoarthritis can occur in any active or non-active individual but usually affects individuals over the age of 50 but can be seen in earlier aged individuals depending on their occupation or their specific sport. When the process of cartilage breakdown begins and progresses, the joint will become stiff and painful.
Above the photo below is a shoulder without osteoarthritis. The space between the upper arm bone and socket still has a maintained joint space.

The picture below is a photo of end-stage osteoarthritis – no space between the upper arm bone and socket.

Post-Traumatic Osteoarthritis
Post-traumatic osteoarthritis is an additional form of the condition that is specifically caused by a traumatic event such as a fracture or trauma such as a shoulder dislocation or repetitive subluxations.
Avascular
Avascular necrosis can also contribute to osteoarthritic changes within the shoulder. This condition is caused by the decrease in blood supply to the head of the humerus (upper arm bone). Without blood supply to a bone, the cells that maintain its strength die. This will cause the collapse of the bone leading to changes within the articular surface and joint. Historically this condition is caused by heavy steroid use, heavy alcohol consumption, and sickle cell disease.
Rheumatoid Arthritis
Rheumatoid Arthritis is a systemic inflammatory condition of the joint lining or synovium. It can affect people of any age and usually affects multiple joints on both sides of the body. Once your physician evaluates you and has determined the possibility of this type of arthritis one will be referred to a specific physician that treats rheumatological diseases.
Symptoms
Symptoms can vary for each individual but specifically start with deep aching pain that can be aggravated by activity. This pain can radiate throughout the shoulder complex as well as into the proximal thoracic (mid-back) or distal cervical spine (lower neck). Snapping, popping and even grinding will be associated with shoulder range of motion that will be decreased compared to a non-arthritic shoulder. Night pain is common.
Diagnosis
Diagnosis will be determined through a thorough history and physical examination by a trained sports medicine and orthopedic shoulder specialist. Examination will consist of palpating the shoulder complex for pain and a visual examination for deformities. The clinician will check both active and passive range of motion and utilize specific manual tests to determine if additional conditions exist. X-rays of the shoulder complex will be ordered to determine the severity of the osteoarthritic changes of the shoulder. Once the initial diagnosis has been made, an MRI (3 dimensional picture) may be ordered to further assist in a complete diagnosis.
Non-Surgical Treatment
Non-surgical treatment or conservative management goals are to decrease painful symptoms allowing individuals improved abilities to perform activities of daily living and labor tasks. Management consists of rest, change in activities, anti-inflammatory (NSAID) medications, Ice 20-30 minutes at times, corticosteroid injections and or medications, physical therapy, and a home exercise program. If you have rheumatoid arthritis, your doctor may prescribe a disease-modifying drug, such as methotrexate, or recommend a series of corticosteroid injections. Dietary supplements, such as glucosamine and chondroitin sulfate (Note: The U.S. Food and Drug Administration does not test dietary supplements. These compounds may cause negative interactions with other medications. Always consult your doctor before taking dietary supplements)
Surgical Management
Surgical management includes several options including shoulder arthroscopy and shoulder replacement. Shoulder replacement is broken down into three procedures, hemiarthroplasty (humeral head replacement), total shoulder replacement (humeral head and glenoid) and reverse shoulder replacement (reversing the ball and socket joint).
- Shoulder arthroscopy, occurs when a small camera is placed into the shoulder joint to visualize the damage. During this visualization, ligaments, bones, and muscles of the shoulder complex are further assessed by the orthopedic surgeon. Once the assessment has been completed the surgeon uses a variety of instrumentation to debride (cleaning) the joint removing loose fragments and performing a Chondroplasty (reshaping of articular cartilage). This is an outpatient procedure.
- Joint resurfacing or resurfacing hemiarthroplasty is performed in young, active individuals with minimal to moderate cartilage erosion. Patients also most have a functioning rotator cuff and intact glenoid cartilage (socket). This open procedure involves placing a prosthetic cap over the surface of the humeral head (upper arm bone). This procedure allows these active patients to retain a similar lifestyle without risking traditional overuse breakdown associated with conventional shoulder stem replacements. This is an outpatient procedure.

- Hemiarthroplasty, replacement of the humeral head or ball (upper arm bone) is replaced with a short stemmed prosthetic containing a metal ball. This procedure is indicated in patients that have moderate to severe cartilage breakdown of the humeral head and minimal to moderate cartilage wear of the glenoid and have intact or minimal damage to the rotator cuff. Hemiarthroplasties are performed in a majority of shoulder replacement candidates. This procedure can be performed at an outpatient surgical center or a short 23-hour observation hospital stay.
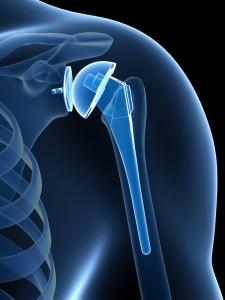
- Total shoulder replacement consists of inserting prosthetic components for both the humeral head (upper arm bone) and glenoid (socket). This procedure is performed for patients that have cartilage wear of both the ball and socket of the shoulder joint and have minimal or no rotator cuff pathology. A short-stemmed prosthesis with a metal ball is placed into the humerus (upper arm bone) and a plastic liner within the glenoid (socket). The prosthetic comes in various sizes and is custom fit to your original shoulder components during the replacement surgery providing the patient new stability and pain-free range of motion. This procedure can be performed at an outpatient surgical center or a short 23-hour observation hospital stay.
Reverse Shoulder Replacement
Reverse Shoulder Replacement is a specialized procedure that is performed for patients that have a chronic rotator cuff tear associated with severe osteoarthritis of the shoulder. When a patient has a non-functioning rotator cuff and severe osteoarthritic pain, the components of the shoulder must be reconfigured. By reversing the configuration of the ball and socket to a socket and ball joint will allow the patient to utilize functioning parascapular (back muscles) and the deltoid to lift the arm while allowing additional pain-free function for activities of daily living. This procedure can be performed in outpatient settings but typically individuals will stay in the hospital overnight being discharged the following day (23-hour observation).

Rehabilitation
Rehabilitation post operatively will begin immediately. Patients will be placed into a sling for 4-8 weeks post-surgical repair. A home exercise program will begin immediately following surgery and formal physical therapy will begin the following day post-operatively. A physical therapist will begin your outpatient rehabilitation through a planned rehabilitation protocol. Initially, the physical therapist will advance pain-free passive range of motion. This pain-free range of motion will be obtained within the first 6-8 weeks. If the procedure is a resurfacing, hemiarthroplasty or total shoulder replacement the rotator cuff will have been repaired and one must allow anatomically healing prior to active strengthening of the shoulder complex. Active motion and strengthening of the shoulder complex will begin around the 16 week post-operative phase per therapeutic protocol. Total recovery from either of the procedures reviewed typically range from 4-8 months.