What is Frozen Shoulder?
Adhesive capsulitis or frozen shoulder occurs when the shoulder joint becomes stiff losing pain-free range of motion. The causes of this condition have been studied are not typically linked to a traumatic event or injury. This condition can occur in anyone but, typically occurs in female and diabetic patients more frequently than men. Additional medical problems such as thyroidism, cardiac surgery, chemotherapy of the chest and immobilization of the arm have also been linked to this condition. About 2% of the population will suffer with adhesive capsulitis of which 10-20% are diabetics.
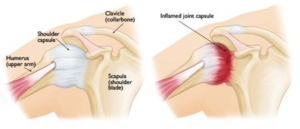
Anatomy
Anatomically, your shoulder complex is a ball and socket joint. It is comprised of 4 main muscles, several bones, and several soft tissue structures. These structures are enclosed by connective tissue called the joint capsule. In adhesive capsulitis or frozen shoulder, this capsule tightens causing symptoms.
Symptoms
Symptoms begin gradually and worsen as the shoulder is moved less and less due to pain. By utilizing the shoulder less, adhesions form within the joint. These adhesions tighten the shoulder causing decreased range of motion and pain with any movement. This is the first stage of the condition called the freezing stage. The second stage, frozen stage, takes place when pain can become severe, a significant range of motion is lost, nighttime pain and the inability to move the shoulder through the full range of motion. The final stage or thawing period occurs when pain decreases and range of motion improves to normal. The process of adhesive capsulitis or frozen shoulder can take over 2 years from onset to resolution.
Diagnosis
Diagnosis will be determined through a thorough history and physical examination by a trained sports medicine and orthopedic shoulder specialist. During the office examination, your shoulder will be moved is all directions to determine what range of motion has been lost. Typically passive and active range of motion has been lost and can be significant at times. Additional manual testing by the specialist will assist in determining the stage of the condition. Occasionally, X-rays of the shoulder complex will be ordered to determine if any bony conditions exist prior to beginning treatment.
Treatments
Treatments can include conservative versus surgical management. A specific individualized treatment program will be created from your thorough history, physical examination, and radiological testing. More than 95% of patients with active adhesive capsulitis will resolve the condition with conservative management. This may take 6-12 weeks to occur once treatment begins. This consists of anti-inflammatory medications, a cortisone injection and physical therapy. Within physical, your therapist will advance range of motion over a 6-8 week period. They will also provide you a home exercise regime that will assist in the daily progression of pain-free range of motion.

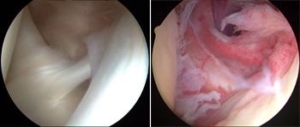
If the range of motion is not progressing conservatively a closed shoulder manipulation would be recommended. Under anesthesia, the physician gently manipulates the shoulder complex in order to tear the adhesions developed and obtain full range of motion. Seldom is arthroscopic surgical management recommend but can occur in patients that have had previous upper arm fractures or previous surgical shoulder procedures. Manipulation and arthroscopic management only occur in 5% of patients. Below, the arthroscopic picture on the left shows normal shoulder tissue. The photo on the right displays adhesions within the shoulder joint, see the redness or tissue irritation.
After shoulder manipulation or arthroscopic debridement, physical therapy is required daily for 1 week then several times per week for 1 month to maintain full range of motion achieved during the procedure. Recovery time varies but usually 6-8 weeks for a closed shoulder manipulation and an arthroscopic debridement and manipulation 10-12 weeks.