What is an ACL Injury and Reconstrcution?
ACL Reconstruction with Hamstring
Surgery performed by Dr. Chams
The knee is the largest and one of the most complex joints in the human body. It consists of 4 bones, multiple ligaments, muscles and tendons, cartilage and soft tissue. Knee ligaments connect bones to bones allowing for stability. Injuries to these ligaments affect more than 12 million people a year requiring visits to orthopedic physicians.
Ligaments
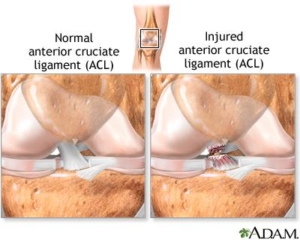
Ligaments of the knee are classified as cruciate and collateral ligaments. Ligaments connect bone to bone. The major ligaments of the knee consist of the ACL (anterior cruciate ligament, PCL (posterior cruciate ligament), MCL (medial collateral ligament) and LCL (lateral collateral ligament). Cruciate ligaments are within the knee joint. They prevent anterior (forward) and posterior (backward) translation of the femur from the tibia.
The ACL is the most commonly injured ligament in the knee complex. Recent studies from 2016 show that nearly 250,000 of these injuries occur per year. Nearly 70% of tears are non-contact injuries – such as a sudden stop, a rapid change of direction or incorrectly landing after jumping. Other studies have shown the female patients have a markedly higher risk of injuring the ligament than male athletes. High-risk sports include gymnastics, skiing, football, basketball, and soccer. Injuries to these ligaments are called tears or sprains. Ligament sprains are classified on a severity scale called grades.
- Grade 1 sprains occur with mild damage to the structure. These injuries continue to keep the joint stable but the ligament is stretched / mildly torn.
- Grade 2 sprains or moderate tears when they occur cause added instability and looseness of the joint. Partial tears at this level may cause episodes or feelings of instability. This grade of injury can be treated without surgery but if typical conservative measures fail then surgery would be recommended.
- Grade 3 sprains or full/complete tears allow for complete joint laxity or no stability. Pending the ligament injury – these grades typically require surgery to remedy.
Signs and Symptoms
Signs and symptoms of injury to this major ligament can occur in a variety of ways including sports, motor vehicle accidents and falls to name a few. Typically the ligament tears with a sudden and rapid change of direction or stopping. It can also occur with direct impact or a compressive force such as landing. Major symptoms within 24hours can include pain, swelling, lost range of motion and instability with walking or attempted return to activity. Some can even feel a tear or pop in the knee when injury occurs.
Diagnosis
Diagnosis will be determined through a thorough history and physical examination by a trained sports medicine and orthopedic knee specialist. Examination will consist of palpating the knee complex for pain and a visual examination for deformities. The clinician will check both active and passive range of motion. Specific manual tests will be performed by the specialist to determine if inflammation exists, the amount of weakness, instability and other possible factors causing symptoms. Once the initial diagnosis has been made, radiological examinations may need to take place for further assessment. An MRI (3 dimensional picture) will be ordered to assist in determining the severity of the ligamentous injury. X-rays of the knee complex may be ordered to determine if any bony conditions exist such as fracture or loose bodies prior to the MRI.
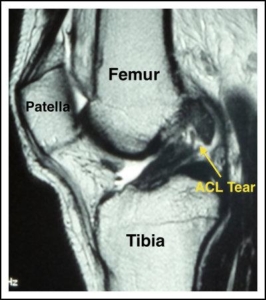
MRI of Torn ACL

MRI of Normal ACL
Treatment
Treatment for an ACL tear can differ pending several factors; age and activity level, osteoarthritic changes and or additional injuries to the knee complex. A specific individualized treatment program will be created from your thorough history, physical examination, and radiological testing. Unfortunately, ACL once torn will not heal without surgical intervention.
- Non-surgical management may be indicated and recommend in cases of isolated tears with no additional derangement for patients that are elderly or for patients that have maintained overall stability of the knee following injury. Conservative management of tears can consist of modification of activity and rest, anti-inflammatory medications, a cortisone injection, orthobiologics such as PRP (platelet rich plasma) or Stem Cell injections, bracing and formal physical therapy.
- Surgical treatment requires either reconstruction or repair of the ligament. Surgical reconstruction or rebuilding of the ligament is most common versus surgical repair. Surgical repair is rarely used as a treatment technique. Repairs are typically only performed when an injury occurs in which the ligament remains intact, but causes a fracture at the site of insertion of the ligament. In this case, the ligament is still attached to the bone fracture. Once the fracture is stabilized through either sutures or surgical hardware the ACL is deemed repaired. Surgical reconstruction requires your surgeon to replace the torn ACL with a tissue graft. These grafts either are autograft (tissue taken from your own body) or allograft (donated human cadaver tissue). Autograft tissue can be acquired either from one of your three hamstring tendons or the middle 1/3 of your patellar tendon from the same affected knee. Allograft tissue can either be from the lower leg (tibialis anterior or posterior), middle 1/3 of a patellar tendon or hamstring. Benefits of each graft choice will be discussed with you during your office examination and a recommendation will be made when all factors have been considered including examination of joint laxity, age, sex, activity level and whether or not this a primary procedure or revision.

Click – Anatomical Video of Arthroscopic Procedure
Click – Surgical Video of ACL Reconstruction
Rehabilitation
Rehabilitation is recommended for both surgical and non-surgical management. Regardless of your treatment choice, your sports medicine physician will determine a personalized treatment program that fits your needs. This recovery process can be long and tasking. However, your active involvement will improve your recovery time. Following the initial onset of signs and symptoms, the initial goal is to reduce swelling and pain, increase mobility and range of motion. At home and at physical therapy, the use of ice, modalities and specific range of motion and strengthening exercises will be performed several times throughout the day. Pain and anti-inflammatory medication may also be prescribed for additional benefit. Crutches and bracing may be initialized following your assessment to aid in stability and prevent further damage to the knee complex. Once reconstruction or repair takes place, physical therapy will begin the following day, working towards restoring full range of motion, strength, and stability of the knee complex. Therapy will consist of visits 2-3 times per week including a daily home exercise program. Advancement to a work specific or sports specific injury prevention program typically occurs around the 3-5 month mark with full return to all activities from 5-8 months.