Biceps Tendinopathy
Open Biceps Tenodesis
3D Surgical Animation
The shoulder complex is a ball and socket joint and is comprised of 4 main muscles, several bones, and several soft tissue structures. The scapula (shoulder blade), clavicle (collar bone), and humerus (upper arm bone) make up the bony components. The primary muscles of the shoulder can be divided into two groups called scapulothoracic and scapulohumeral. The scapulothoracic muscles help stabilize the shoulder complex to the thoracic spine or mid back are comprised of the trapezius, rhomboids and serratus anterior. The scapulohumeral muscles consist of the main movers of the shoulder joint the rotator cuff and deltoid. The rotator cuff (supraspinatus, infraspinatus, teres minor and subscapularis) and deltoid work together to provide additional stability and function to the shoulder complex.
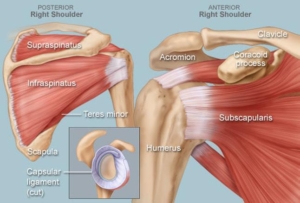
A portion of your scapula called the glenoid articulates with the head of your humerus. To stabilize the ball and socket articulation, strong fibrous tissue called the labrum, deepens this socket. In addition to the labrum, capsular ligaments attach around the joint to create additional stability and function.
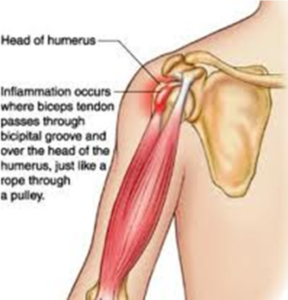
Inflammation of Biceps Long Head

Proximal Long Head Attachment
The biceps muscle is located in the front of your arm. It has two upper (proximal) tendons that attach within the shoulder. The long head of the biceps attaches to the superior portion of the labrum and the supraglenoid tubercle as seen in the photo above. The short head of the biceps attaches to the coracoid process. The function of your biceps at the shoulder is to assist with humeral head stability with resistance to torsional forces. Within the short and long heads, the short is rarely damaged or torn. However, the long head of the biceps is a common area of pain within the front of the shoulder complex. Proximal biceps tendonitis is the inflammation of the cord like band, the biceps tendon, that connects the biceps to the shoulder. Chronic proximal biceps tendonitis can lead to biceps tendon rupture.
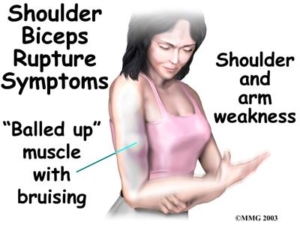
Signs and Symptoms
Signs and symptoms associated with proximal biceps tendonitis include pain and tenderness in the front of the shoulder or into the biceps, lost strength, pain with rotation of your shoulder, popping of the shoulder with rotation or with reaching away from your body. With a Biceps rupture, similar symptoms will appear as with tendonitis, but one may notice a biceps bulge, feel a pop when the injury occurs and notice swelling and discoloration throughout the upper portion of the arm. This is referred to as a “popeye arm.”
Diagnosis
Diagnosis will be determined through a thorough history and physical examination by a trained sports medicine and orthopedic shoulder specialist. Examination will consist of palpating the shoulder complex for pain and a visual examination for deformities. The clinician will check both active and passive range of motion. Specific manual tests will be performed by the specialist to determine if inflammation exists, the amount of weakness and other possible factors causing symptoms. An ultrasound machine may also be used within the office assessment to evaluate the painful pathology. Once the initial diagnosis has been made, an MRI (3 dimensional picture) may be ordered to confirm the diagnosis and assist in determining the severity of the injury. Occasionally, X-rays of the shoulder complex will be ordered to determine if any bony conditions exist prior to your MRI.
Treatment
Treatment goals are to increase strength, decrease pain and improve the functionality of the shoulder complex. These results can be obtained through either conservative or with surgical management. A specific individualized treatment program will be created from your thorough history, physical examination, and radiological testing.
- Conservative management of tendonitis and partial thickness tears can consist of a modification of activity and possibly rest, anti-inflammatory medications, a cortisone injection, orthobiologics such as PRP or Stem Cell injections and formal physical therapy. If conservative treatment was attempted for partial thickness tears or chronic tendonitis and symptoms have not improved or resolved, then surgical intervention would be recommended by the specialist.
- Surgical management for both partial and full thickness tears may be recommended pending the severity of the tear and any other additional pathology associated with the current condition of the shoulder complex such as a rotator cuff tear or labral tear. Surgical management consists of two options for patients, tenotomy, and tenodesis. Tenotomy occurs when the biceps tendon is cut from its attachment site within the shoulder complex and allowed to roll or bulge in the arm. This bulge is a permanent deformity and results in occasional cramping post operatively. A tenodesis also is a result of cutting the long head of the biceps from its attachment site. Conversely, the biceps tendon is then reattached just outside the shoulder joint removing the inflamed or diseased portion from the shoulder complex. Regardless of either option functionality of the shoulder will not be compromised.

Click here for subpec biceps tenodesis procedure
Conservative Rehabilitation
Conservative Rehabilitation for tendonitis and partial tendon tears will begin following your initial assessment. A cortisone injection may be offered to reduce pain and inflammation. Formal physical therapy should begin immediately to gain range of motion, stability, and strength. Use of modalities by the therapist such as ultrasound and electrical stimulation may also be used to assist in improving the function of the shoulder complex. IN additional to physical therapy, the exercise clinician will provide a detailed home exercise program to continue to develop strength, stability and maintain range of motion. Many with just tendonitis improve symptoms quickly. Those with partial tears may take several months for improvement.
Surgical Rehabilitation
Surgical Rehabilitation will begin immediately. Patients will be placed into a sling for 3-4 weeks depending on any additional procedures performed during the surgical repair. A home exercise program will begin immediately following surgery. These exercises will be performed until formal rehabilitation can begin one to two weeks following surgery. A physical therapist will begin your formal rehabilitation through a planned rehabilitation protocol. Initially, the physical therapist will advance pain-free passive range of motion. This pain-free range of motion will be obtained within the first several weeks. During this time, some strengthening will occur including parascapular and isometric strengthening of the rotator cuff.